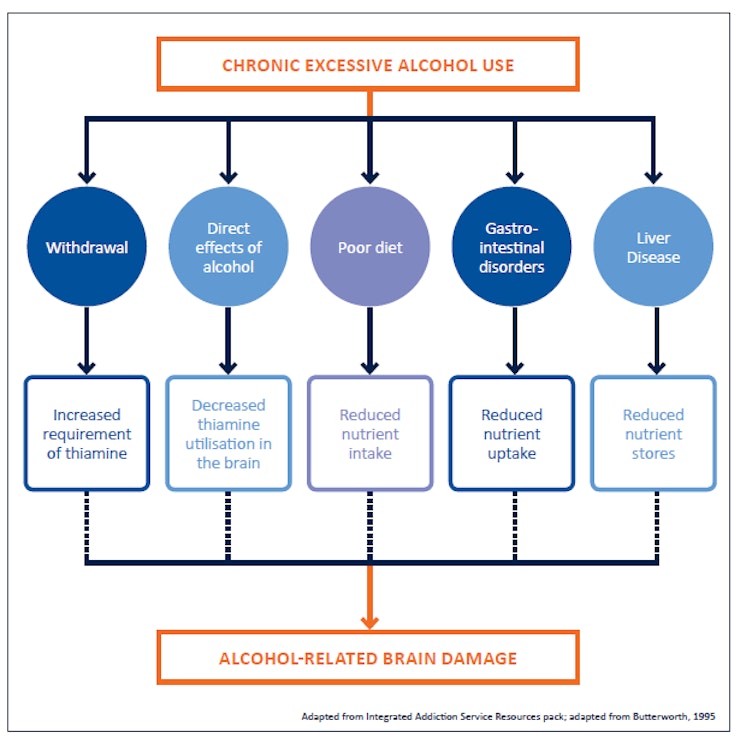
Alcohol-related brain damage is an umbrella term for conditions affecting the brain caused by long-term excessive alcohol use. For men, that's 50+ units of alcohol a week, and for women it's more than 35 units of alcohol a week for a period of five years or more. In terms of drinks, that equates to 5 bottles of wine or 20 pints of lager in a week for a man, and just less than 3½ bottles of wine or about 14 pints of lager per week for a woman. The recommended maximum alcohol use for adults (men or women) in the UK is 14 units per week, ideally spread over three or more days and with at least two alcohol-free days each week.
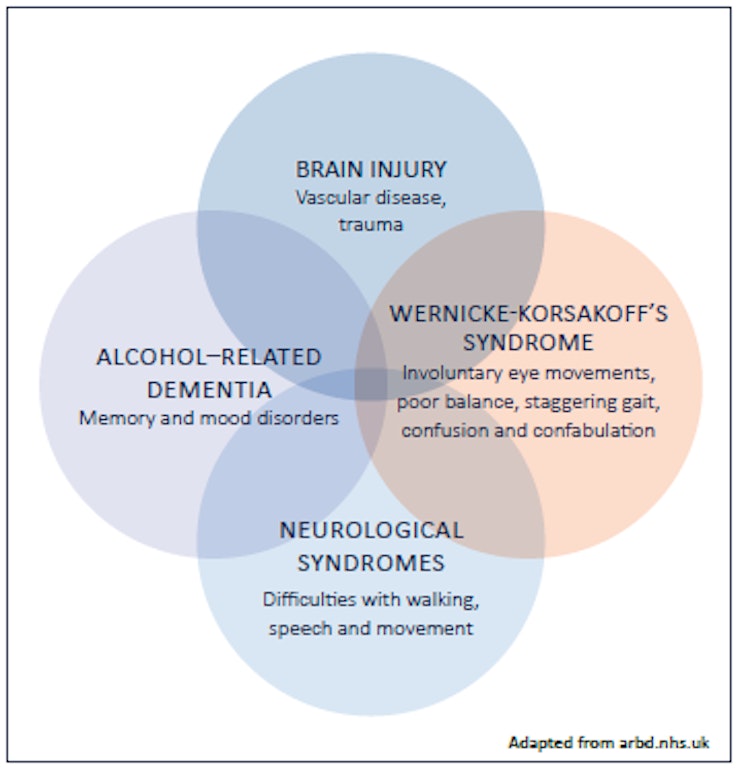
Research suggests that around 35% of dependent drinkers have some form of ARBD. Many patients will exhibit symptoms of more than one type of ARBD, with around 25% also showing signs of other brain trauma. This can make accurate diagnosis more difficult.
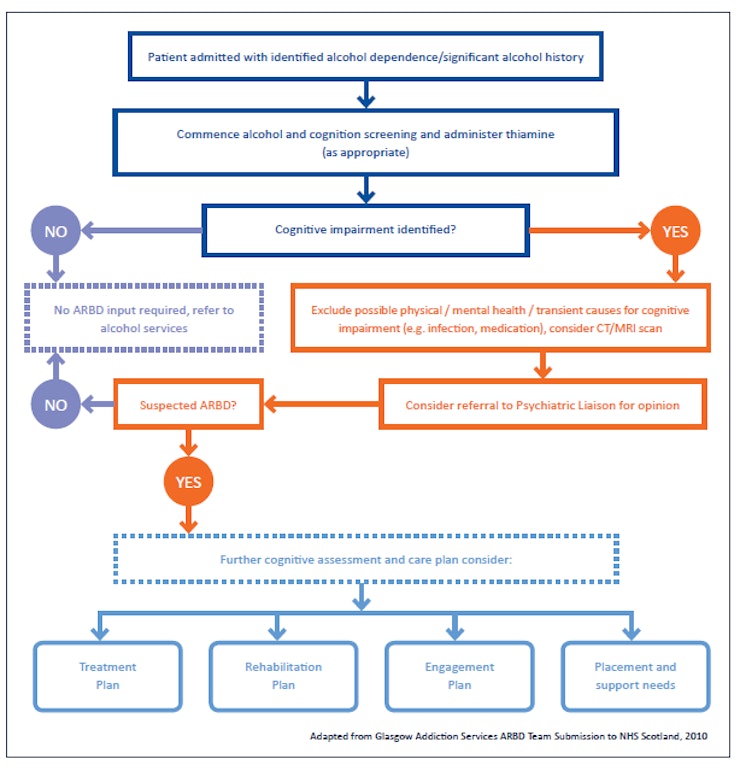
Many of these conditions are treatable (for example, around 75% of people with Wernicke-Korsakoff’s Syndrome will recover to some extent). So, early diagnosis is important. If you suspect that someone you are working with has alcohol-related brain damage, they should be strongly encouraged to speak to a medical practitioner or you should seek permission to do this on their behalf.
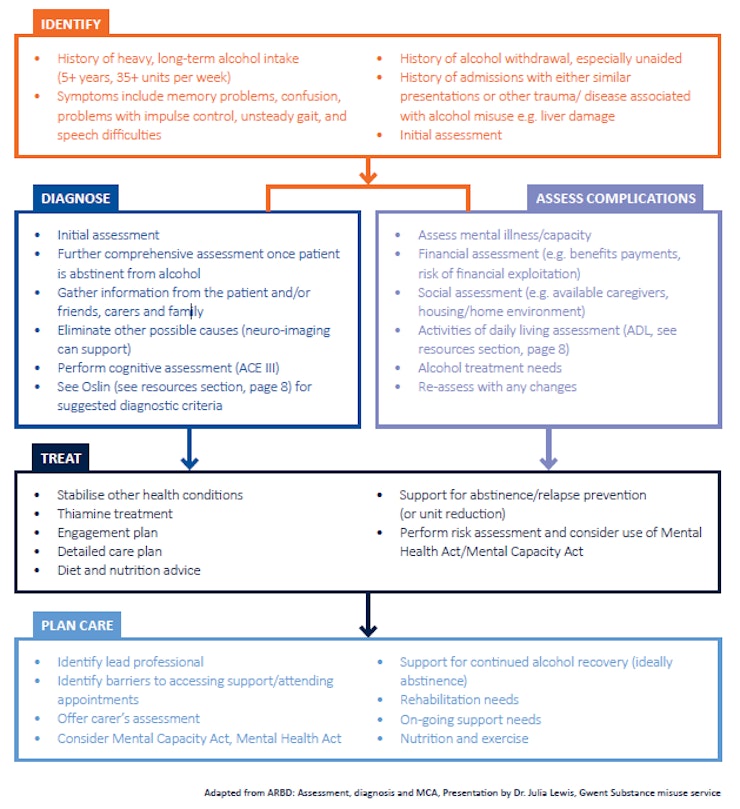
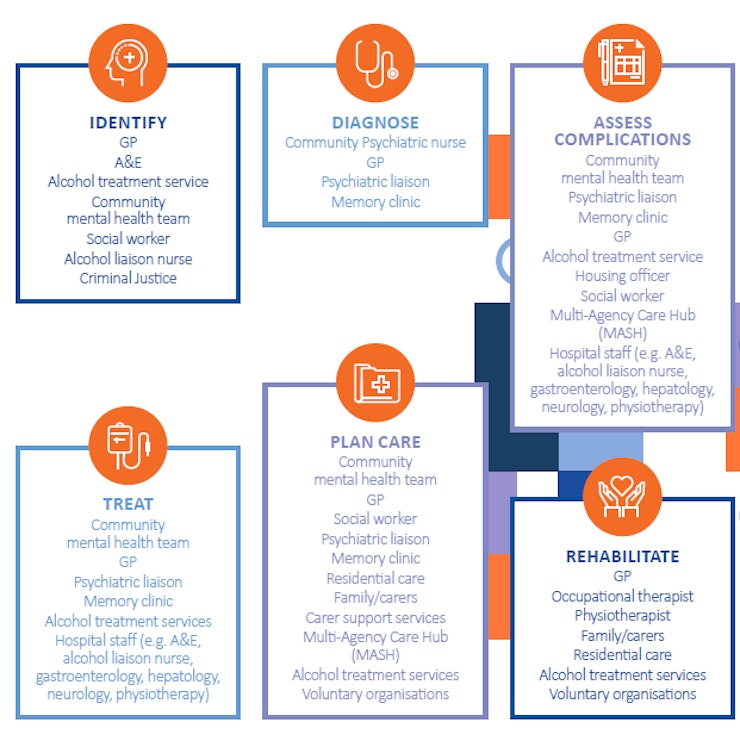
Often, patients will have complex health and social care needs. A multi-agency approach, lead by a key worker and supported by outreach work has been found to be the most effective in helping people with ARBD to achieve their maximum potential for recovery.
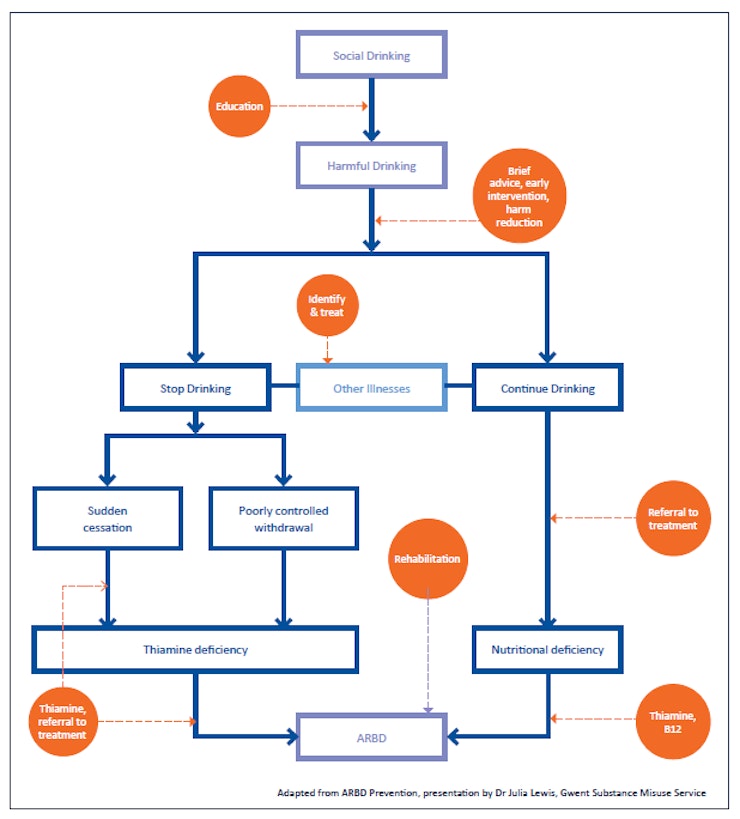
Anyone at risk of ARBD should be encouraged to take preventative measures such as reducing their alcohol unit intake, improving their nutrition and attending regular health check-ups.